Case report
- Information for veterinarians
- Indications
- Rehabilitation and fitness training
- Case Report
- ESVN Paris 2013
- ESVN-ECVN Symposium 2014 - Madrid
- Glossary
Veterinary Orthomanual Medicine in a Dachshund with posterior paralysis
Heukels J, Aharon DC
Summary
An 8 year old dachshund was presented for evaluation of acute posterior paralysis and loss of bladder control. The diagnosis of thoracolumbar intervertebral disc disease (TLDD) grade IV was made clinically. Additional diagnostics and surgical options were declined by the owner. The dog was treated with veterinary orthomanual therapy (VOT), followed by cage rest. At the two week follow-up the dog was ambulatory, but paraparetic, and had intact bladder control. At the six week follow-up, the dog was clinically and neurologically normal. This case report illustrates VOT as an effective, non-invasive and cost-effective treatment for dogs with TLDD.

Introduction
Acute spinal cord injuries related to the intervertebral disc are common in chondrodystrophic dog breeds. In this Hansen type-1 intervertebral disc disease, chondroid degeneration precedes a protrusion or extrusion of the nucleus pulposus or annulus fibrosis.5,8,20,35 Extrusion or protrusion can cause compression, contusion and ischemic damage to the spinal cord and nerve roots.20,32 The thoracolumbar region is predisposed to intervertebral disc disease (TLDD).24,35
During the initial phase, the extruded intervertebral disc causes damage to the spinal cord by compression and contusion. Disruption of cell membranes and impediment of spinal perfusion and drainage induce ischemic neuronal and glial injury, and damage to myelin and axons. The primary phase initiates a series of secondary destructive mechanisms, including rapid changes in ion concentrations, production of free radicals, inflammation, excitotoxicity (excessive neurotransmitter stimulation), and destruction of the microvascular bed.20,32
The clinical manifestation of TLDD depends on the degree of gray and white matter spinal cord compression, caused by primary and secondary trauma. Symptoms vary widely between individuals and may include local pain, paraspinal muscle hypertonicity, and pelvic limb neurological deficits.2,7,20 Pain is the result of irritation and compression of the meninges and nerve roots.10,20,24,35
The neurological state, evaluated according to the severity of neurological deficits, is classified as follows: 20,24,34
| Grade | Neurological state | Proprioception | Bladder control | Deep pain perception |
|---|---|---|---|---|
| I | Pain | + | + | + |
| II | Paraparesis | - | + | + |
| III | Paraparalysis | - | + | + |
| IV | Paraparalysis | - | - | + |
| V | Paraparalysis | - | - | - |
Treatment options for clinical TLDD are conservative, e.g. cage rest and anti-inflammatory medication; non-surgical, e.g. physiotherapy23,26 and acupuncture21; and surgical.7,20,24,26,28,32 Manual treatments, such as orthomanual therapy, are regularly used to treat back problems in humans4,39 and veterinary orthomanual therapy (VOT) has also been practiced for several years.1
Orthomanual medicine assumes that intervertebral disc degeneration causes vertebral instability. This instability can induce misalignment of consecutive vertebrae. Vertebral misalignment, instability and intervertebral disc degeneration result in extrusion or protrusion of the nucleus pulposus or annulus fibrosus. Spinal cord compression and trauma due to kinetic energy of the extruded intervertebral disc can cause pain and neurological deficits.39 It is theorised that correcting the misalignment of the vertebrae diminishes the pressure on the intervertebral disc and creates an environment that facilitates an improvement in the neurological state.1
CASE DESCRIPTION
Signalement and history
An 8 year old male dachshund (12.6 kilograms) was presented at the Practice for Veterinary
Orthomanual Medicine in Noorden with acute onset back pain and pelvic limb paralysis. Symptoms appeared one day earlier and were of acute onset. Prednisolone-sodium succinate (Solu-delta-cortef; 50 mg IV and 50 mg SC) was administered by the referring veterinarian on the day of onset, and cage rest was prescribed. Urinary catheterization was performed to relieve urinary retention. The owner was given instructions to perform urinary catheterization 4 times a day at home.
Two years earlier, the dog had fully recovered from an acute spinal problem with pelvic limb paralysis grade IV after receiving orthomanual treatment. One year later, the dog was briefly and successfully treated with non-steroidal anti-inflammatory medication and rest for lameness of the right hind limb because of a painful hip joint.
Clinical findings
The dog was presented with posterior paralysis. No abnormalities were noted on the general physical exam. The orthopaedic examination and testing of the spinal reflexes were performed on the dog in left- and right-sided lateral positions. The right hip joint was painful and easily subluxated upon forced abduction.
The muscle volume and tone of all limbs were normal. The m. extensor carpi radialis (C7-Th2), withdrawal (C6-Th2) and triceps reflex (C6-Th1) of both thoracic limbs were intact. The patellar (L3/4-L6), withdrawal (L5-S1) and cranial tibial reflex (L6-S1) of both pelvic limbs were intact.38 The perineal reflex (S1-S3) was intact. Superficial and deep pain perception were intact in all limbs. Proprioceptive positioning (knuckling) was absent in both pelvic limbs.33 The bladder was of normal size and not easily evacuated by manual abdominal pressure.
Neuroanatomical localization and differential diagnosis
Summarized findings on the neurological examination were: symmetrically absent proprioception of the pelvic limbs and intact spinal reflexes of the thoracic and pelvic limbs. Proprioceptive deficits indicate an upper motor neuron symptom (UMN) and a spinal cord lesion located cranially from the segment innervating the concerning limb. The normal spinal reflexes indicate intact reflex arcs and corresponding spinal segments. Therefore, the lesion must be located between Th3 and L3, and classifies as grade IV.
Differential diagnosis of acute Th3-L3 spinal cord lesions are: TLDD, trauma, and fibrocartilaginous embolism. Complementary diagnostics with myelography, computed tomography (CT) of magnetic resonance imaging (MRI)6,7,24 and subsequent surgery were advised. The owner renounced further diagnostic options and chose a non-surgical treatment.
Orthomanual examination and treatment
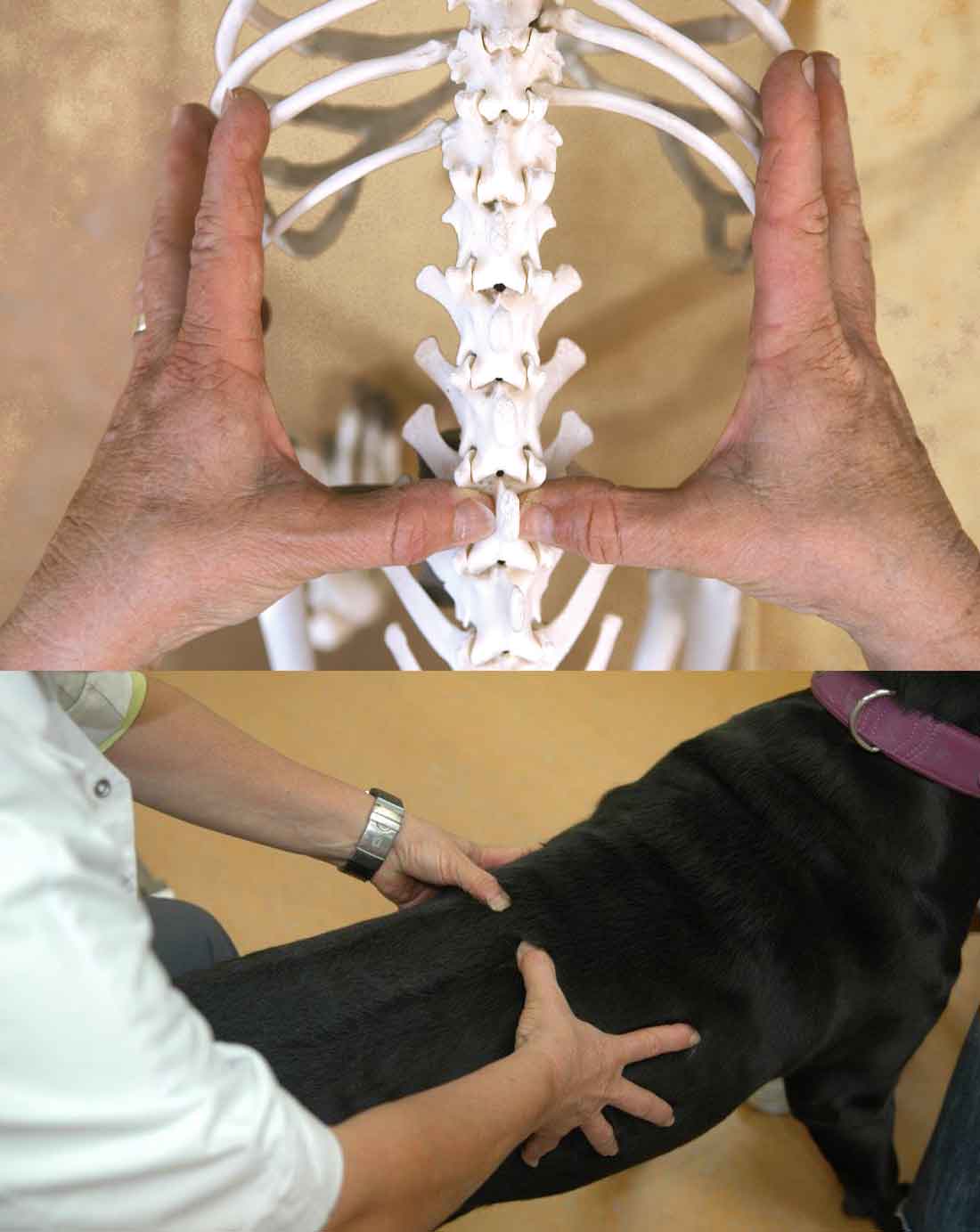
The orthomanual examination is performed on the dog standing squarely in front of the veterinarian. The dog's body is supported by an assistant, using both hands. The vertebral column is palpated from tail to head by placing the thumbs on either side of the vertebral dorsal spinous process. Vertebral misalignment is detected by visual inspection of the position of the thumbs and by palpation. Asymmetry, local pain and paraspinal muscle tone, as well as muscle atrophy are noted. A misaligned vertebral position is corrected by slightly elevating the vertebral body with the thumb and then imparting an impulse to the spinous process with the thumb, thereby pushing it into the correct position.1 Misaligned vertebrae generally require little force to be pushed back into their original positions, because it is applied in the direction of the natural position or function.39
The orthomanual examination revealed local pain and an increased muscle tone at the level of Th11, Th12, and Th13. Furthermore, misalignment of Th11, Th12, and Th13 was detected and corrected. Cage rest during 14 days was prescribed.40
Follow-up and prognosis
During follow-ups, the orthopaedic, neurological and orthomanual examinations were repeated. At the two week follow-up, the dog was ambulatory with posterior paresis. Proprioception was intact in the right hind leg, and impaired in the left pelvic limb. The dog was pain-free and had regained full bladder control. In the following four week rehabilitation period, a gradual increase in freedom of movement, combined with cage rest in between activities was prescribed.24,35
At the six week follow-up, the dog's gait was completely normal and proprioception was intact in both pelvic limbs (neurological grade 0). The orthomanual treatment was therefore considered successful and completed.
Discussion
The diagnosis of TLDD is often based on the patient's signalement and history, symptoms, and findings on the physical examination. Considering the neuroanatomical localization and the acute onset in this patient, TLDD is the most probable diagnosis.32 The first clinical episode of TLDD typically occurs between the age of 3 to 7 years.7,20 This agrees with the dog's age at the time of his initial posterior paralytic condition.
Recurrence of TLDD, regardless of the treatment method, is a well known phenomenon.7,12,28 The recurrence rate after surgical treatment is 2-15%. Dachshunds are three to ten times more likely than other breeds to have recurrent symptoms.12,15,19,31 In most cases, this is caused by extrusion or protrusion of an intervertebral disc adjacent to the original site. The recurrence rate of TLDD after conservative treatment is 30-50%.20,24 Data on recurrence rates after VOT are lacking. From practical experience, it is presumed that the mean interval between a first and a recurrent episode is longer after VOT in comparison with surgical treatment. The reason for this might be that surgery causes local decompression, whereas VOT corrects all misaligned vertebrae, including those at sites of subclinical intervertebral disc disease.
A fibrocartilaginous embolism (FCE) is the main differential diagnosis for this dog. However, FCE typically occurs in large breeds and often results in asymmetrical neurological deficits.11,17 Additional diagnostics are required to confirm the diagnosis, but these bear additional risk for the animal (e.g., if anaesthesia is required) and higher costs for the owner.7,10,24
Orthomanual therapy in dogs with TLDD is presumed to create a condition that facilitates improvement of the neurological state by relieving pressure on the intervertebral disc and spinal cord.3,39 The misalignment of the 12th and 13th thoracic vertebrae in this dog corresponds with the TLDD predilection sites in chondrodystrophic breeds. These are Th12-Th13 and Th13-L1.28,34,37 In the retrospective study of Aharon and Buntsma, which evaluates the efficacy of VOT in 261 dachshunds with presumptive TLDD, misaligned positions were also most commonly found at Th12, Th13 and L1.
Subsequent cage rest allows the healing of ligamentous structures and the partial resorption of extruded disc material. It also prevents further extrusion. Enforced rest also reduces the probability of accidental traumatic injury in ataxic dogs. 14,23,36
The conventional treatment of TLDD grade IV is surgical. The surgery aims to decompress the spinal cord and remove the extruded intervertebral disc material. The traditional approach is hemilaminectomy.7,30 Other procedures, such as minihemilaminectomy and pediculectomy, aim to achieve spinal cord decompression through less invasive techniques and by removing less vertebral bone.7,25,27,28,29
Efficacy studies of TLDD treatment methods define and categorize the clinical effects differently.24 To summarize, most studies refer to clinical, rather than neurological recovery. In these cases, the criteria for a successful treatment are: 1) unassisted walking, and 2) improvement of the neurological state. Residual pain or paresis are not taken into account. Thus, with regard to neurological state, patients with residual grade II and grade III neurological deficits are generally considered as successfully treated. 18,20,22,23,31 Review of literature reveals a 46-100% success rate for surgical treatment 8,20,24,25,28,31,35, and a 50-54% success rate for conservative treatment23,34 of TLDD grade IV.
Differentiation between assisted and unassisted walking patients reflects the assessment of the animal's quality of life as it is made by the owner, and is appropriate for that purpose. However, lack of uniformity in the evaluation of TLDD treatment efficacy makes comparison of studies difficult.
In Aharon and Buntsma's study, neurological recovery is assumed and progress is graded. A successful treatment is defined as recovery to grade 0, which means lack of residual pain or paresis. The success rate of VOT in dogs with TLDD grade IV, according to these standards, is 48%. Furthermore, the condition of 43% of dogs improved, going from grade IV to grade I (ambulatory, pain-free, with intact, delayed proprioception, or with some residual motor deficiency). In the neurological evaluation, proprioception is considered intact or absent. It is common for the clinician to interpret a delayed proprioceptive reflex as well. Restoration of proprioception is the final phase of recovery.24
This case report illustrates the clinical and neurological recovery of a dog with posterior paralysis after VOM treatment. Two weeks after the treatment, the dog was ambulatory and the neurological state improved from grade IV to grade I. Six weeks after the treatment, the dog was ambulatory with a normal gait and intact proprioception in both pelvic limbs (grade 0).
In conclusion, veterinary orthomanual medicine is an effective, non-invasive treatment method for dogs with TLDD. VOT is cost-effective and minimally stressful for the patient. In addition, the complication risk is absent. Comparison of efficacies of different treatment methods for TLDD is difficult. There is a need for definition and uniformity in the evaluation of success.
Abbreviations
FCE: Fibrocartilaginous embolism
LMN: Lower motor neuron
MRI: Magnetic resonance imaging
TLDD: Thoracolumbar intervertebral disc disease
UMN: Upper motor neuron
VOM: Veterinary orthomanual medicine
VOT: Veterinary orthomanual therapy
Acknowledgments
The authors would like to thank Dr. Luc Janssens and Prof. E. Gruys for their advice.
Literature:
- Aharon DC, Buntsma RF. Orthomanual therapy for treatment of suspected thoracolumbar disc disease: A retrospective study. Gepresenteerd op het 24th Annual Symposium of the ESVN Neurological Genetic Diseases, september 2011, Trier Germany.
- Anderson DK, Means ED, Waters TR, et al. Microvascular perfusion and metabolism in injured spinal cord after methylprednisolone treatment. Journal of neurosurgery 1982;56:106-113.
- Assendelft WJJ, Lankhorst GJ. Effectiviteit van manipulatieve therapie bij lage rugpijn: geen uitsluitsel in systematische literatuuroverzichten en behandelrichtlijnen. Nederlands tijdschrift geneeskunde 1998;142:684-688.
- Balthazard P, De Goumoens P, Rivier G, Demeulenaere P, Bellabeni P, Dériaz O. Manual therapy followed by specific active exercises versus a placebo followed by specific active exercises on the improvement of functional disability in patients with chronic non specific low back pain: a randomized controlled trial. BMC Musculoskelet Disord. 2012 Aug 28;13(1):162.
- Bray JP, Burbidge HM. The canine intervertebral disk. Part Two: Degenerative changes-nonchondrodystrophoid versus chondrodystrophic disks. Journal of the American Animal Hospital Association 1998;34:135-144.
- Bos AS, Brisson BA, Nykamp SG, Poma R, Foster RA. Accuracy, intermethod agreement, and inter-reviewer agreement for use of magnetic resonance imaging and myelography in small-breed dogs with naturally occurring first-time intervertebral disk extrusion. J Am Vet Med Assoc. 2012 Apr 15;240(8):969-77.
- Brisson BA. Intervertebral disc disease in dogs. Vet Clin North Am Small Anim Pract. 2010 Sep;40(5):829-58.
- Coates JR. Intervertebral disk disease. The Veterinary clinics of North America. Small animal practice 2000;30:77-110.
- Da Costa RC, Moore SA. Differential diagnosis of spinal diseases. Vet Clin North Am Small Anim Pract. 2010 Sep;40(5):755-63.
- De Lahunta A, Glass E. Veterinary neuroanatomy and clinical neurology, 3rd ed. 2009. St. Louis, Saunders/Elsevier, pp. 243-248.
- De Risio L, Platt SR. Fibrocartilaginous embolic myelopathy in small animals. Vet Clin North Am Small Anim Pract. 2010 Sep;40(5):859-69.
- Dhupa S, Glickman N, Waters DJ. Reoperative neurosurgery in dogs with thoracolumbar disc disease. Vet Surg. 1999 Nov-Dec;28(6):421-8.
- Dietz V. Neuronal Plasticity After Spinal Cord Injury: Significance for Present and Future Treatments. J Spinal Cord Med. 2006; 29(5): 481-488.
- Doita M, Kanatani T, Ozaki T, Matsui N, Kurosaka M, Yoshiya S. Influence of Macrophage Infiltration of Herniated Disc Tissue on the Production of Matrix Metalloproteinases Leading to Disc Resorption. Spine 2001;26: 1522-1527.
- Forterre F, Gorgas D, Dickomeit M, Jaggy A, Lang J, Spreng D. Incidence of spinal compressive lesions in chondrodystrophic dogs with abnormal recovery after hemilaminectomy for treatment of thoracolumbar disc disease: a prospective magnetic resonance imaging study. Vet Surg. 2010 Feb;39(2):165-72.
- Fries CL, Remedios AM. The pathogenesis and diagnosis of canine hip dysplasia: a review. Can Vet J. 1995 August; 36(8): 494-502.
- Gadeyne C, De Decker S, Van Soens I, Bhatti S, Van Meervenne S, Martle V, Saunders J, Polis I, Van Ham L. Fibrocartilagineus infarct: een retrospectieve studie van 57 verdachte gevallen. Vlaams Diergeneeskundig Tijdschrift,2007,76,117-123.
- Hayashi AM, Matera JM, Fonseca Pinto AC. Evaluation of electroacupuncture treatment for thoracolumbar intervertebral disk disease in dogs. J Am Vet Med Assoc. 2007 Sep 15;231(6):913-8.
- Hettlich BF, Kerwin SC, Levine JM. Early Reherniation of Disk Material in Eleven Dogs with Surgically Treated Thoracolumbar Intervertebral Disk Extrusion. Vet Surg. 2011 Nov 21. doi: 10.1111/j.1532-950X.2011.00920.x.
- Jaggy A, Platt SR. Small animal neurology. An illustrated text. 1st. ed. Schlütersche, Hannover, 2010.
- Janssens LAA, Prins EMD. Treatment of thoracolumbar disc disease in dogs by means of acupuncture: a comparison of two techniques. Journal of American Animal Hospital Association 1989;25:169-174.
- Joaquim JG, Luna SP, Brondani JT, Torelli SR, Rahal SC, de Paula Freitas F. Comparison of decompressive surgery, electroacupuncture, and decompressive surgery followed by electroacupuncture for the treatment of dogs with intervertebral disk disease with long-standing severe neurologic deficits. J Am Vet Med Assoc. 2010 Jun 1;236(11):1225-9.
- Levine JM, Levine GJ, Johnson SI, et al. Evaluation of the success of medical management for presumptive thoracolumbar intervertebral disk herniation in dogs. Veterinary Surgery. 2007;36:482-491.
- Lorenz MD, Coates JR, Kent, M. Handbook of veterinary neurology (5th ed), Saunders/Elsevier, St. Louis, (2011), pp. 75-77.
- Lubbe AM, Kirberger RM, Verstraete FJM. Pediculectomy for thoracolumbarspinal decompression in the dachshund. J Am Anim Hosp Assoc 1994;30:233-8.
- Mann FA, Wagner-Mann CC, Dunphy ED. Recurrence rate of presumed thoracolumbar intervertebral disc disease in ambulatory dogs with spinal hyperpathia treated with anti-inflammatory drugs: 78 cases (1997 - 2000). Journal of Veterinary Emergency and Critical Care 2007;17:53-60.
- McCartney W. Partial pediculectomy for the treatment of thoracolumbar discdisease. Vet Comp Orthop Traumatol 1997;10:117-21.
- McKee WM. A comparison of hemilaminectomy (with concomitant disc fenestration) and dorsal laminectomy for the treatment of thoracolumbar disc protrusion in dogs. The veterinary record 1992;130:296-300.
- Moissonnier P, Meheust P, Carozzo C. Thoracolumbar lateral corpectomy for treatment of chronic disk herniation: technique description and use in 15 dogs. Vet Surg. 2004 Nov-Dec;33(6):620-8.
- Muir P, Johnson KA, Manley PA, Dueland RT. Comparison of hemilaminectomy and dorsal laminectomy for thoracolumbar intervertebral disc extrusion in dachshunds. J Small Anim Pract. 1995 Aug;36(8):360-7.
- Necas A. Results of surgical treatment in disorders of the thoracolumbar disks in dogs. Vet Med (Praha). 1995 Jul;40(7):213-6.
- Olby N. The pathogenesis and treatment of acute spinal cord injuries in dogs. Vet Clin North Am Small Anim Pract. 2010 Sep;40(5):791-807.
- Rijnberk A, van Sluis FJ. Anamnese en lichamelijk onderzoek bij gezelschapsdieren. Bohn Stafleu van Loghum, 2005, p.205-207.
- Scott HW. Hemilaminectomy for the treatment of thoracolumbar disc disease in the dog: a follow-up study of 40 cases. The journal of small animal practice 1997;38:488-494.
- Sharp NJH, Wheeler SJ. Small animal spinal disorders, diagnosis and surgery. London: Mosby-Wolfe Publishers 2005; 12.
- Simpson ST. Intervertebral disc disease. The Veterinary Clinics of North America. Small Animal Practice. 1992;22:889-897.
- Tanaka H, Nakamaya M, Takase K. Usefulness of myelography with multiple views in diagnosis of circumferential location of disc material in dogs with thoracolumbar intervertebral disc herniation. The journal of veterinary medical science 2004;66:827-833.
- Thomson CE, Hahn C. Veterinary Neuroanatomy - A Clinical Approach. Elsevier Health Sciences, 2012. Chapter 13: Neurological examination and lesion localization.
- Van de Veen EA, de Vet HC, Pool JJ, et al. Variance in manual treatment of nonspecificlow back pain between orthomanual physicians, manual therapists, and chiropractors. Journal of manipulative and physiological therapeutics 2005;28:108-116.
- Wheeler SJ, Sharp NJH. Small animal spinal disorders, diagnosis and surgery. London: Mosby-Wolfe Publishers 1993; 8-18, 30, 85-108.